
When a father testifies in court that no bed was available in a psychiatric unit for his mentally ill 15-year-old son, who then went on to try to murder a woman, you might wonder which children do occupy those beds and how they are admitted.
While the public will never know the exact circumstances of that individual case, the boy's father told the Court of Appeal last month that he regretted his son had not been hospitalised. The court increased the review date for the teenager's 11-year sentence by two years, to seven years, after finding that the original five-year term was too lenient for his attack on Stephanie Ng at the Dún Laoghaire seafront in December 2017.
A report published by the Health Research Board (HRB) last month, compiled by Antoinette Daly and Sarah Craig, profiles the under-18 intake to Irish psychiatric units last year.
Behind the statistics, how does the inpatient system work – or not in some cases – for children with mental health disorders who need intense treatment?
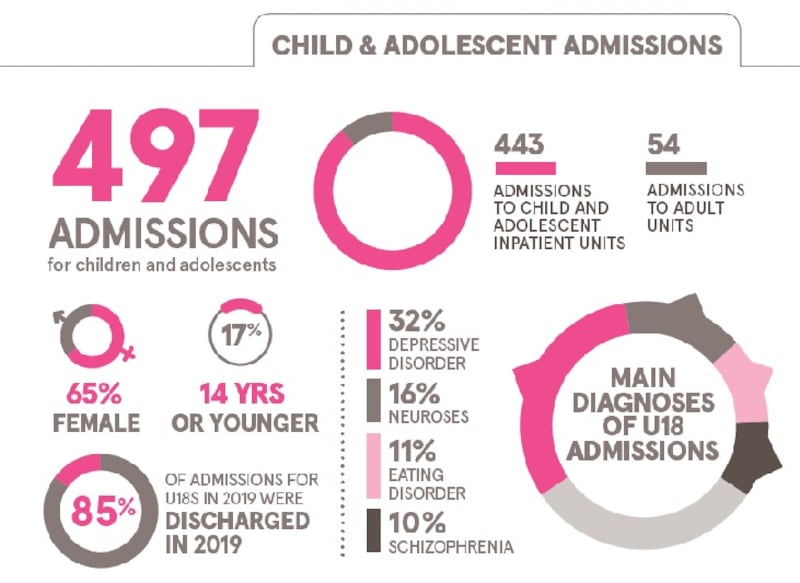
The number of under-18 admissions to psychiatric inpatient facilities was 497 last year, up 89 from 2018
This is not necessarily bad news. While nobody likes to think of a child with a mental health disorder so serious that they need to be taken away from family and community for residential treatment, this rise can be mostly attributed to the doubling of capacity at one of the four public units – Linn Dara, in Cherry Orchard Hospital, Dublin.
A knee-jerk, "Oh my God it's terrible" reaction to increased numbers is, suggests Linn Dara's clinical director Prof Brendan Doody, "stigmatisation of children requiring inpatient treatment". Such treatment is very helpful, he points out, and "it is not an asylum".
However, 54 of the admissions were to adult psychiatric units – a practice that the Ombudsman for Children's Office has described as "unacceptable". The only positive thing about that figure is that it was 30 fewer than the previous year. Nearly half of those 54, spread between 15 adult units, were soon transferred to Child and Adolescent Mental Health Services (CAMHS) units, where they are in effect "double counted" as they would be recorded as new admissions.
The Mental Health Commission says children and young people should not be admitted to adult units "except in exceptional circumstances". Its recently published annual report for 2019 says that because there are only three counties (Dublin, Cork and Galway) with inpatient CAMHS units and only two of these units have out-of-hours admissions, "children and young people in crisis are left with the unacceptable 'choice' between an emergency department, general hospital, children's hospital or an adult inpatient unit".
Meanwhile, what goes unrecorded, say critics of the system, are the children who arrive in crisis at hospital emergency departments and have to be admitted for care and treatment of psychiatric illness because no beds can be found for them in a psychiatric inpatient unit. The Mental Health Commission deals only with admissions to “approved centres” under the Mental Health Act.
So how many CAMHS beds are available around the country?
On paper, there are 98, of which 72 are in the four HSE-funded units: Linn Dara in Ballyfermot, Dublin (24 beds); St Joseph’s at St Vincent’s, Fairview, Dublin (12); Eist Linn, Bessborough, Co Cork (16) and Merlin Park, Galway (20). In addition, there are two private units in Dublin: Willow Grove, St Patrick’s Mental Health Services (14) and the Ginesa Suite at St John of God’s Hospital, Stillorgan (12). But, and it’s a big but, these are not all operational at any one time, due mainly, it is said, to staff shortages.
Would there be enough beds if they did operate to full capacity?
No. Back in 2006, the Vision for Change document for reform of the country’s mental health services over the next decade recommended just over 100 public beds in dedicated units for children and young people. We’re inching towards that, again on paper, with 10 secure beds due to open in Portrane, Co Dublin, next year and a further 20 earmarked for the new children’s hospital, be that in 2023 or 2024, or beyond.
An updated Sharing the Vision framework for the next 10 years, which was published in June, says that while there has been an increase in CAMHS beds since the original policy was drawn up, “there have been some challenges in accessing sufficient age-appropriate inpatient beds, exacerbated by staff availability issues and complexity of cases”. It highlights the “need to consider” capacity and operation of beds throughout the mental health services.
“A review needs to take place,” agrees Doody, who is also a clinical associate professor at Trinity College, Dublin, not just into the numbers but the types of beds available. There has been significant population growth since 2006 and the provision of 100 beds is low by European standards. Increases here were coming from a very low base – there were only 14 CAMHS beds in 2008.
However, of course more beds aren’t the whole answer either; many more resources are needed in the community to help prevent children’s mental health issues escalating to crisis level. There are persistently well over 2,000 children and young people on waiting lists for CAMHS services in the community, as increased investment is offset by rising need.
Mental Health Reform has pointed out that despite the HSE implementing a "very intensive waiting list initiative", there was only a 3.9 per cent decrease in numbers, from 2,541 in 2014 to 2,440 by August last year.
“The better the services in the community, obviously less children will end up being referred to inpatients and the quicker you are able to discharge them,” says Doody.
How does the “accessing” of beds work?
Each of the HSE units has a primary catchment area for referrals but any of them can take children or teenagers from outside their areas for specialist treatment, such as that for eating disorders at Linn Dara and Merlin Park. Patients with private health insurance can be referred to either of the two private units.
There is a “triage of referrals”, says Doody. Each unit looks at its capacity and options and may contact another unit to pass on a referral. There is a weekly national telecall between the units to discuss any waiting lists.
Despite the appearance of co-operation, there is criticism that the public units tend to operate as “silos”. One consultant psychiatrist working outside the inpatient units argues that the appointment of an overarching bed manager would bring more transparency and greater fluidity to availability of resources.
About 60 per cent of referrals are admitted after a screening process. Maybe the condition doesn’t merit inpatient admission or it is decided that it wouldn’t be helpful for the child, Doody explains.
In response to the raising of the testimony of the father of the boy involved in the Dún Laoghaire attack, he says while he would prefer not to comment on an individual case, “in general terms, if a child at a particular time is not assessed as meeting the threshold for admission, it doesn’t mean they couldn’t be referred in a week later and meet the threshold”.
Lack of clarity about such a “threshold” is a contentious issue with some psychiatrists working outside the units. After all, referrals to the units can only be made by consultant psychiatrists who judge that their patients need inpatient treatment and who must fill in a very lengthy form outlining their case. Yet in four out of 10 cases, it seems their opinion is being overruled by colleagues inside the units.
The HSE’s operational guidelines published in 2019 covering admission to CAMHS inpatient units are more extensive on what’s not appropriate for referral than what is appropriate. In making clear that the final decision on admissions rests with the inpatient consultant psychiatrist, they say that those accepted will, “in general, have a severe and complex mental disorder which requires the level of treatment provided in an inpatient setting”.
There has to be “clear evidence” that this level of intensive treatment is required and that “there is a level of risk due to their mental disorder that is more appropriately managed in an inpatient setting”. That risk can be to themselves and/or others.
When it is decided not to admit, the parents and referring doctor are supposed to be informed of the reasons in writing. This doesn’t always happen, according to one psychiatrist who in one case, despite repeated efforts, could not get any information beyond the fact that the referral had not been accepted.
For what conditions are the under 18s being admitted?
Almost a third of the patients are diagnosed with depressive disorders (32 per cent), the next most common group are neuroses, ie anxiety disorders (16 per cent), followed by eating disorders (11 per cent) and schizophrenia (10 per cent). While all units will admit any of the above, they say they vary in their abilities to manage challenging behaviour, which indicates there are fewer options for these difficult cases.
Specialist beds for eating disorders at Linn Dara and Merlin Park include the facility for nasogastric (ng) feeding as part of a treatment programme for anorexia.
How long do they stay in?
While nearly one in five is discharged within one week of admission, the median length of stay at a CAMHS unit is 34 days. Those with eating disorders, for instance, are likely to need to be there longer.
However, although the average inpatient stay is 42 days, they are unlikely to be in the unit all that time as the measure is from date of admission to discharge. There will be “therapeutic leave”, ranging from a few hours out to an overnight away.
“You don’t want to break that connection with home,” says Doody and leave is also “a way of gauging how much progress the young person is making”.
What ages are most of these patients and what’s the gender divide?
More than a third of admissions (37 per cent) are aged 17 and a quarter (27 per cent) are 16. However, with children as young as 11 being admitted with eating disorders, 6 per cent of all inpatients are aged 13 or younger.
Females account for 67 per cent of all admissions; they make up 95 per cent of those with an eating disorder, up from 85 per cent in 2018, according to the HRB figures. Girls are also predominant among those with depressive disorders or neuroses, while males account for 87 per cent of admissions with a diagnosis of other drug disorders and 67 per cent of those with schizophrenia.
Is it a medical model of care?
While the ultimate responsibility for an inpatient lies with a consultant psychiatrist in a unit, the approach is multidisciplinary, and teams include nurses, psychologists, speech and language and occupational therapists, social workers, dietitians and teachers. The school attached to Linn Dara is “a really important part of the inpatient treatment programme”, says Doody, as almost invariably school attendance has broken down before a young person is admitted and it may have become a significant stressor in their lives.
Is inpatient treatment successful?
It depends on how you define success. The goal from the day of admission is discharge. “Success is you don’t have to be an inpatient anymore,” says Doody. Units are focusing on the change necessary for a child or teenager to continue treatment as an outpatient.
For example, inpatient treatment for anorexia is targeted at weight gain, restoring a child to a more normal weight range, “but you still leave the unit suffering from anorexia”.
Inpatient treatment needs to be used judiciously “and it is not without its negative aspects”, he warns. It can be unhelpful, for example, for those with severe behaviour difficulties; for emotional disorders, brief admission can be helpful but prolonged admission not so.
“You’re treating a child and a family, you’re not treating a condition,” he adds. “It is about individual care plans, individual goals. Really the goal is to have to have as short admission as possible.”
“There are no emergency services in paediatric psychiatry in this country”
There are huge inequities in how the health system treats a child with a potentially life-threatening physical illness such as asthma and an equally serious mental health disorder, according to paediatric consultant psychiatrist Dr Kieran Moore.
The child with asthma attends a GP in the first instance and, in more serious cases, may need to go to hospital outpatients; if it’s really bad, they will be admitted.
At the emergency department it doesn’t matter if there is a bed available or not, they will get a bed if they need it, he says, speaking in a personal capacity to The Irish Times. Hospitals will immediately co-operate on transfers by ambulance in such an emergency if needs be.
If a young patient with a mental illness needs to be admitted, they are first seen by the GP, who will know of the huge waiting lists for CAMHS in the community, so instead they go to a hospital emergency department.
Doctors in A&E have very little psychiatric training, Moore points out, and while the child may be admitted to a paediatric ward and looked after to the best of the staff’s abilities, “there is no safety in terms of the Mental Health Act, no review of their admission, and this is for primary psychiatric reasons”.
The system’s handling of such emergency cases is akin, he argues, to telling an asthma patient there are no beds available but they could try the psychiatric hospital down the road. The young patient with life-threatening asthma will always be treated but a “ridiculous amount of work” has to go into trying to get inpatient psychiatric treatment for their peer with a mental illness, even when there’s a risk to life.
“There are no emergency services in paediatric psychiatry in this country,” he adds. The current system of stand-alone units “goes away from the acuteness that people are sick, and they are not being treated in a quick and timely fashion in my view”.











