

In 1989 a young social care worker named Bernard Gloster took a temporary job for two months as a caretaker in the Southill Health Centre in Limerick city. He will go back there soon to switch on its Christmas lights – now returning as the boss of 150,000 people who work for the Health Service Executive (HSE).
It is nine months tomorrow since this now 57-year-old Limerick man became chief executive of the health and social care service. Not surprisingly, considering his early career, he is careful to name both aspects when talking about the HSE.
“Social care often gets set aside because of the visibility of the ‘trolleys’,” he remarks, in reference to the catchword in people’s minds for a health service in crisis. We’re heading into what is traditionally peak “trolley season” in the country’s hospitals, but the new man at the helm has scrapped the accompanying ritual of a HSE winter plan.
“Every day is a winter, to some degree, when we talk about trolleys,” says Gloster, in his first, wide-ranging media interview about his priorities and ambition for change in the pressurised HSE.



We’re sitting in a meeting room of the 18th-century Dr Steevens’ Hospital in Kilmainham, Dublin 8, which stopped functioning as a hospital in 1987 and is now HSE HQ. It is only a few minutes’ walk away from the office he occupied as chief executive of Tusla, the Child and Family Agency, for the previous three and a half years.
Up to now, his sporadic media engagements have been driven by single issues, the highest profile of which was going out to bat on RTÉ Radio 1 on the Sunday after Budget Day to say the allocation of additional funds for health was not adequate. This, along with his warning that any attempt to make the HSE break even would cause harm to patients, was reportedly not appreciated in Government circles.
“The health budget always makes a few headlines. It probably made a few more this year than previously, but that’s the way it is,” he smiles. There is nothing flashy or bombastic about Gloster, whose entire career has been in the public service, but there is a hint of steeliness in his eye contact which suggests he is not to be messed with. “I have challenging conversations with lots of people every day,” he says at one point, “because of my impatience to make it better.”
But he says he’s a listener too. “I invest at least one of my days a week connecting with the people who matter. The people who matter are the people who want the service – and the people who give the service.”
In addition to official trips to HSE services, he makes unannounced visits alone. He spent the Sunday afternoon before we talk walking around the three hospitals at the “epicentre” of the recent Dublin rioting – the Rotunda, CHI at Temple Street and the Mater – chatting to staff. These, of course, included workers from other countries, some of whom have an anxiety now, he points out, about whether Ireland was the right place to come to work.
A week does not pass without him meeting a member of the public who has had experiences of the health service – “some of it good, some of it not good”. He can’t meet everyone who writes to him, but he has a staff member whose job it is to look out for stories they can learn from. Recent contacts have included sitting in the kitchen “of somebody considered a high-profile case in the country” and reaching out to parents of children with eating disorders who staged a protest outside the Department of Health over the lack of treatment available.
Earlier in the year, Gloster met patient advocate John Wall, who is living with a serious cancer diagnosis, and then invited him to address the entire HSE senior management team. Speaking to Clare FM afterwards about this “unprecedented” opportunity, Wall said a sea change was needed within the health services and he believed it was beginning to happen.
“I am operating on the principle that change in public service is complex, but not impossible,” Gloster says. He believes he has to be the type of chief executive that straddles both the “now” and the “next”. The “now” because “people can’t wait”, and the “next” because he also needs to deliver on medium- to long-term strategic planning.
When bringing senior staff together very early on, he reminded them of the pseudonym of “Mrs O’Neill” that was used in a policy document some years ago – for a 79-year-old widow who has two chronic illnesses and lives alone. “All she wants is good quality healthcare from professionals who talk to each other. I keep saying to every part of the health system that Mrs O’Neill’s request is not unreasonable.”
Yet, “we have made responding to her request very complex”.
He came into the job promising “the most significant delayering of the HSE”, and will finish that process this week with the appointment of six regional executive officers, as conceived by Sláintecare. But he has arranged that each will report directly to him, eliminating two layers of the current, equivalent chain of command.
Organisational restructuring, while potentially hard for staff, is of little interest, he acknowledges, to users of the health and social care services. More relevant is the three areas he has chosen to focus on for now:
Access to hospital services
“I call it access and performance because the two are related,” Gloster says. He is talking here about both non-scheduled and scheduled care, which is where trolleys and waiting lists respectively come in. After abandoning the notion of a winter plan, he told staff there had to be an all-year-round effort to reduce times people spend on hospital trolleys. There has already been a big improvement in waiting times for people over 75, he says.
“A lot of the narrative of last winter was people over 75 spending 24, 36, 48, 72 hours on a trolley, and I have read some of their stories. There is no doubt at times that experience is something you could only be ashamed of.”
He has been accused of lacking ambition in saying that no one over 75 will wait more than 24 hours, but he believes it is “not a bad place to start”, considering what has been going on. “It is not that we are happy for people to wait 24 hours – [we’re] just saying we have zero tolerance for over 24 hours. But we are striking well under that already.”
Gloster has also been criticised for reiterating that remaining in hospital after treatment is not “a choice to be exercised” by older people awaiting their preferred option of long-term care. He says he respects people’s wishes, “but I am also very pragmatic. If I can’t give somebody their first choice, I sure as hell am not going to allow them to lie in a hospital bed when they don’t need to be there, deconditioning.” It is a question of appropriateness of care as well as “a patient safety issue for the person at the other end trying to get into the hospital”.
He is also keen to highlight the inroads the HSE is making into reducing waiting lists. While the numbers attract the headlines, the critical factor, he stresses, is the length of time people are on waiting lists.
He takes the most recent full month of October at time of interview as a snapshot, looking back two years for a comparison. In October 2021, there were 644,458 people on the waiting list (spanning all specialities), and the average waiting time was 12.6 months. “Some people are waiting four years and some people waiting three months, but that was the average.”
In October this year, there were 588,813 on the waiting list, with an average waiting time of 8.1 months. This was “despite massive new referrals beyond what was expected”. It is still a long way from the Sláintecare target of 10 weeks’ wait, he concedes, but “we are certainly a lot further on than we were”.
He believes there is a need to change how people get on to waiting lists. Currently, GPs often refer to a consultant they know. “I very much want to move to a position where our hospital groups have a central referral system. So if you need an ENT [Ear Nose and Throat] appointment, your GP refers you to the group for ENT and the group distributes among all the ENT consultants depending on where you’ll get the best time to wait to be seen.”
That would obviously be more efficient, “but you would be amazed how hard it is to achieve it because it is not the way our system is used to working, and people will resist it”.
Timely implementation
“I kept explaining to senior managers it was the ‘timely’ part of that that was the issue,” says Gloster who has made timely implementation a second priority. He reckons the HSE is very good at policy development and planning, but too slow to act.
“By the time we usually get to implementation, the issue of the efficacy of what we are doing has come into question. Either it is not consistently rolled out or it has taken too much time. You see that in things like e-health.”
Public confidence
Public confidence was something Gloster worked on restoring in Tusla and is now keen to address at the HSE. “Coming here, I heard all the good stories about the health service, and it’s such a pity most people don’t hear them.” Currently, there is no bandwidth or airtime for the positives, he says, because of the access and implementation problems. “I wouldn’t blame people.”
While the health services are under pressure “and it’s hard graft for everybody working here”, he believes they are making progress. He can tell the public they will improve the trolley situation and, although “we can’t fix it all today, the other thing that is fundamentally important to me is to improve the experience of people while they are waiting”.
Money matters
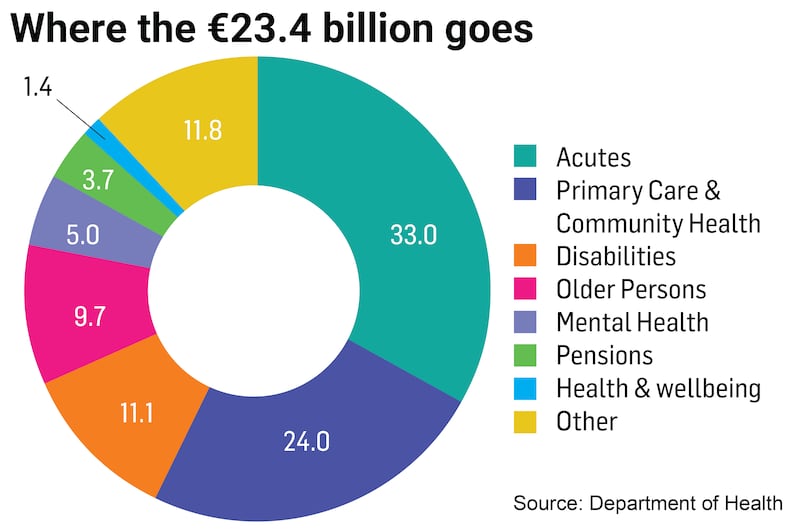
Eight weeks on from the announcement of Budget 2024, Gloster recaps on what it means for the HSE, which had a record budget of €23.4 billion this year, serving a population of 5.1 million. Next year, the service will have all the funding it had for healthcare this year, plus an additional €700 million “to help us keeping doing what we are doing today – and that is a really good thing”. There is also €100 million for new developments or pre-existing commitments. This ensures, for instance, that it will be able to staff the 22 new ICU beds it is in the middle of building. That is a total of €800 million additional core funding: “It will come in and stay.”
The HSE has also received approximately €1 billion in non-core funding as a once-off towards the 2023 deficit to account for continuing fall-out from Covid, the effects of the conflict in Ukraine and some of the health-related inflationary pressures that far outstrip general price inflation.
While he had warned that if the Government required the HSE to break even next year, it would cause harm because services would have to be cut, he says now: “I am being very clear that the Government has not asked me to do that, and I don’t believe they will ask me to do that. I believe what they will ask me to do is demonstrate the best level of productivity for the public interest from the money we have, and then let’s see where we go.”
But he also stresses that “the impact of the challenge we have next year means we have to slow down the rate of growth of development of services. We won’t be progressing all of our programmes at the same rate as we were previously, and we had banked on doing a lot of that.
“I am still hopeful that I am going to convince them that the budget is worth investing more in as we go through next year.” However, “to be fair to the Minister for Public Expenditure, I do have to start the year not aspiring to reach a deficit. I have to start aspiring to the lowest level of deficit possible.
“We have a serious amount of money. There is waste and there is lack of control in part, but I would say it’s the smaller part of the challenge – but it’s the one part I can deal with.” This need to control is “why the taxpayer pays me the enormous amount of money that I’m paid”.
His annual salary is €352,023.
Recruitment freeze
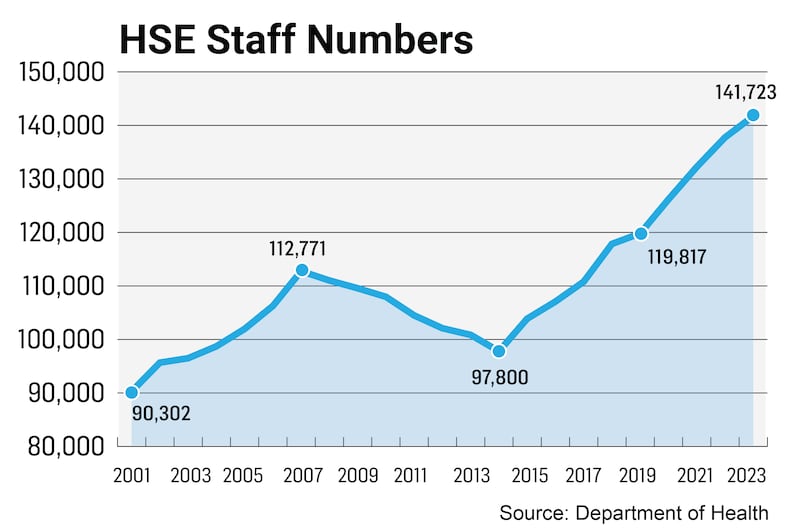
The HSE was funded for an additional 6,100 staff this year. Gloster introduced a “recruitment pause” when he saw two months ago that the HSE was going to hit and exceed that total before the end of the year. There has been industrial action and political and public criticism in response. “All of that is for other people to deal with. We have had the biggest ever workforce in the history of the health service.”
There is a workforce of almost 142,000 whole-time equivalents (WTEs), involving about 150,000 individuals. “My job is to use that to best effect. Could I do with more? Of course, absolutely. I would be lying to say I didn’t need more, but I can do a lot with what I have.”
[ No cuts to health services next year despite ‘guaranteed deficit’, HSE chief saysOpens in new window ]
There is funding for an additional 2,208 staff in 2024, but that means they are going to go into the year challenged. “I intend to give every hiring area, eg hospital group, community healthcare organisation area, a funded workforce, within which they will have X amount for WTEs, X for overtime and X for agency workers. As long as they operate within the totality of that, they won’t be part of any arbitrary nationwide decision to cap if somebody else goes off line.”
Recruitment challenges
While there is often talk of the difficulty the HSE has in filling jobs, he says the 23,000-person net growth in the workforce since the start of 2020 would not indicate that. However, there are “certain services that are difficult to recruit for”. These include psychiatry, an internationally competitive market, and there are 75 vacancies in this area. He hopes the public consultant contract will help put a dent in that shortage.
“Lots of people said nobody would sign it and over 1,000 people have signed it so far, so I am hopeful but guarded on that.” He also says they are “significantly challenged” in the hiring of allied health professionals, such as occupational therapists, physiotherapists and speech and language therapists, “particularly for disability”.
Gloster is also concerned about the dependency in nursing and some medical disciplines upon people trained abroad. He values what staff from other jurisdictions bring to our services, but “the problem for us is eventually our level of dependency would be so significant if we keep growing at the rate we are that it is not sustainable. You must also act ethically when doing international recruitment; the countries a lot of people come from also require their professionals.”

Additional training places need to be created here for all health and social care disciplines. While there is a “credible argument” for introducing minimum service requirements for professionals educated here, he has a hesitancy about how it would work in practice. If somebody does not want to stay here, “what would their quality of care be like to Mrs O’Neill on a trolley at two o’clock in the morning?”
In his conversations with young health professionals about to emigrate, “not everyone says, ‘Why would you stay in the HSE?’; some would say, ‘Why would you stay in Ballybunion when you can have Bondi?’”
Integrated care
Services and specialities not connecting with each other is a general criticism of the HSE – none more so than in child and adolescent mental health. He acknowledges Camhs (Child and Adolescent Mental Health Services) is under great pressure, but points out there are many more specialised teams than previously. “I think the professional community would say we still don’t have everything we need and I accept that, but I don’t accept we are always doing everything to the best degree we can with what we have. Usually for me that comes back to integration.
“I never met a young person who needed Camhs and never needed anything else. The more we specialise, the more in danger we are of defining that [the] child doesn’t need us – he needs somebody else. Well, the child needs us to find the somebody else.”
Everybody has to chip in to be part of the solution. “If we can start there, I think a lot more parents would feel safer – and feel safer for their children.”
Challenge of ageing population
“I have a real moral and ethical dilemma about how we talk about older people in terms of our health services because, no matter how well intended we are, we often make them feel they are part of the problem,” he says.
While we “thankfully” have had the best improvement rate in life expectancy in Europe, “we haven’t quite cracked the quality of life in those latter years”. The percentage of the population over 65 is expected to have almost doubled, to 26 per cent, between 2019 and 2051. The numbers over 85 are projected to treble over the next 20 years.
“We can’t wake up in Ireland in 20 years’ time and say we didn’t know this was coming.” Meanwhile, the “now” has to be about the best level of homecare services, aids and appliances that can be provided to enable people to stay at home. Investment is needed in rehabilitation services, respite care and in long-term care. There also has to be far more planning for dementia.
Personal responsibility
Gloster is troubled by the very poor uptake of Covid boosters and the flu vaccine, even among healthcare workers who interact with so many vulnerable people. He is clearly angry at what he terms the “very small but very negative, serious anti-vaccine influence out there”. That is totally different from “vaccine hesitancy”, which he can understand, say, among new parents of babies.
“When I hear the absolute diatribe that is the sort of thing that destroyed the HPV vaccine a few years ago, and it took somebody like the late Laura Brennan to help us correct that... I have no tolerance for the disinformation and the abuse that goes on about flu vaccine and Covid vaccine.”
To him, it is obvious why people should not just protect themselves but everybody around them. “Personal responsibility is a thing and personal responsibility about how we use valuable public services is a thing.”
Occupying the hot seat
Gloster feels “enormously privileged” to have the role of chief executive. “You get the chance to influence and you only get it for a very short time.
“I try to be reasonably healthy,” he adds. “I might be a bit tired at times but I am paid to be tired.”







