
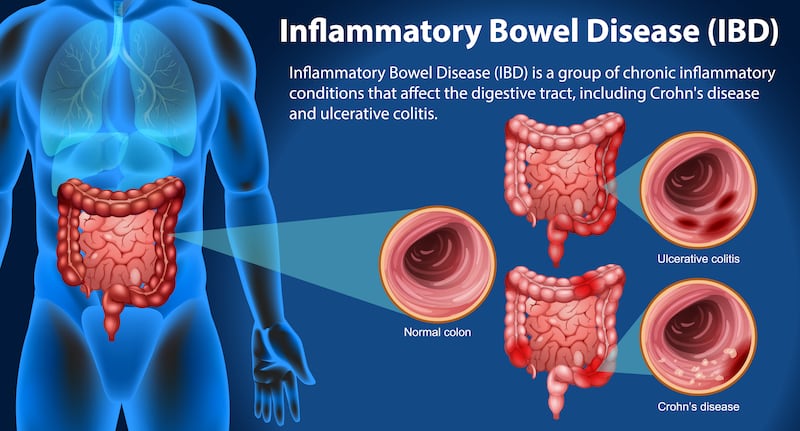
Inflammatory bowel disease (IBD) – the group of chronic conditions that causes inflammation, swelling and ulceration of the small and large intestines – has been on the rise in Ireland, Europe and North America in recent decades. But now studies are showing that countries across Asia and South America are also showing increased incidence of Crohn’s disease and ulcerative colitis – the two most common types of IBD – as western-style diets take hold in these regions.
“There is lots of epidemiological evidence to show that the western diet is implicated in the development of IBD,” says Majella O’Keeffe, registered dietician and senior lecturer in human nutrition and dietetics at University College Cork (UCC).

She explains how, as countries become more economically developed and industrialised, researchers are observing in real-time the so-called “nutrition transition” as diets move away from the less-refined traditional diets to western-type diets with higher amounts of fat, sugar and processed foods. O’Keeffe will speak at the Crohn’s and Colitis Ireland conference for people with IBD from noon to 6pm on Sunday, May 19th, in the Kingsley Hotel, Cork city.
Dr Cara Dunne, consultant gastroenterologist at St James’s Hospital and Children’s Hospital Ireland (CHI) at Crumlin, says she has noted a doubling of cases of young people diagnosed with IBD in the last 10 years or so. “There are two peaks in the diagnosis of IBD – in the early teens and in those aged 40 onwards,” says Dunne. “Genetics is a factor, but then there is an environmental trigger which gives rise to ulcerative colitis and Crohn’s at a certain point.”
READ MORE




Changes in the gut bacteria from the overuse of antibiotics and the over-consumption of ultra-processed foods made with preservatives, emulsifiers and stabilisers are among the culprits which are most associated with the rise in these chronic bowel conditions. “Certain food additives such as emulsifiers have been linked to IBD,” says O’Keeffe. “Research has found that emulsifiers in particular may increase the pro-inflammatory bacteria in the gut which disrupts the mucous in the intestines.” Emulsifiers are added to processed foods to improve consistency and lengthen the shelf-life of products.
And while efforts to replace ultra-processed foods with wholefood diets could arguably be part of a wider strategy to reduce the incidence of IBD – and other chronic conditions – the Mediterranean diet, which has high amounts of fruit and vegetables, wholegrains, lean meats, fish, nuts and pulses and Omega-3 fats (from fish or supplements), can also be part of the treatment for the condition outside of flare-ups.
Emily Farrell, who was diagnosed with ulcerative colitis about 10 years ago, does her best to avoid processed foods. “I try to stick to non-processed foods in my diet and I take vitamin D, vitamin C and iron supplements,” explains the 22-year-old.
Pains in her stomach and blood in her stools were the first signs that something wasn’t right for the then 12-year-old girl from Blanchardstown. “I remember being in primary school and thinking maybe if I skip breakfast, my stomach won’t hurt, so I would do just that and that turned into skipping my lunch in school as well.”

Her GP initially prescribed laxatives, thinking that she was suffering from constipation. But when, one day, her mum noticed a significant amount of blood in the toilet after Emily had a bowel movement, alarm bells were raised. “Diarrhoea – particularly nocturnal diarrhoea, blood in the stools, anaemia and weight loss are red flags for IBD,” explains Dunne, adding that while the less serious irritable bowel syndrome also has symptoms of diarrhoea and constipation, this condition is not driven by an inflammatory process.
Further tests, including an endoscopy at CHI Crumlin, resulted in a diagnosis of colitis for Emily. She was put on medication to treat the condition, which worked for a number of years. “It completely changed my life. But, five months ago, I changed to a new injectable medication because I was fatigued and my eczema got so much worse. Now, I have more energy and my skin is better,” she says.
Dunne says that medications to treat IBD have become much more sophisticated in recent years as specialists now have a choice between a range of biologics/biosimilars, immune-modulators and so-called small molecules. “These drugs dampen down the immune response so that complications don’t occur. Most people do well on medication, but patients need to be seen every six months to monitor and change their medications if necessary.”
Smoking and excess alcohol consumption cause more severe symptoms of IBD. And exacerbations of symptoms of IBD can result in hospitalisation and in some severe cases require emergency surgery to remove part of the intestine. “Up to 25 per cent of patients with ulcerative colitis will require some surgery in their lifetime. Some patients with limited forms of Crohn’s disease can actually benefit from surgery and not require further treatment afterwards.”
Emily remembers how as a teenager she experienced an exacerbation of her symptoms: “I had a flare-up when I was 14 and was admitted to hospital where I very narrowly escaped having to get a colostomy bag.” She completed her degree in business, marketing and law in 2023.
During flare-ups, some people with IBD – and children in particular – are given medically prescribed liquid formula instead of food or the so-called beige diet (bland foods with low-fibre content) for a period of time to allow the gut to rest and recover.
In terms of access to diagnosis and treatment, the scarcity of dieticians in multidisciplinary teams is cited by O’Keeffe as a cause for concern. “There is a big shortage of specialist IBD dieticians so patients are often given dietary advice by the IBD specialist nurse or other members of the team,” she says. Studies have shown that patients with IBD are at risk of anaemia and general malnutrition and that malnourished patients are more likely to have flare-ups, be admitted to hospital, suffer from severe infections, and have longer hospital stays and more post-operative complications.
Gastroenterologists would also like to see more GPs carrying out initial diagnostic tests to identify IBD in patients. This would result in faster access to colonoscopies for those who need them and less unnecessary colonoscopies for those who don’t.
There are two specific tests that GPs could use to fast-track patients needing urgent referral. These are the faecal calprotectin test which monitors the enzyme calprotectin whose levels increase in white blood cells when inflammation occurs.
The faecal immunochemical test, which is already used in colon cancer screening programmes, picks up blood in the stools at levels unseen by the human eye. The risk of colon cancer is also higher in people with IBD so the faecal immunochemical test would also be very useful to detect early-stage cancers for those who aren’t in the age bracket for colon cancer screening programmes. GP access to laboratories for results of such tests remains an issue in some parts of the country.
- Sign up for push alerts and have the best news, analysis and comment delivered directly to your phone
- Find The Irish Times on WhatsApp and stay up to date
- Listen to our Inside Politics podcast for the best political chat and analysis









